Clinical Trials
and
Case Reports
Clinical Trials
Clinical Trials and Studies
![]()
For decades, electromagnetic therapies have shown clinical effectiveness in treating neurologically-related diseases, wound healing, and bone repair. In this section, we present the clinical trials and pilot studies thus far conducted using Stimpod NMS460 for the treatment of diabetic neuropathies, intractable pain, and migraine.
{kind=link}
{kind=link}
Clinical Trial: Diabetic Neuropathy
(Randomized, single-blind, placebo-controlled)
(Randomized, single-blind, placebo-controlled)
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind, randomized placebo-controlled trial.
P. Berger1, S. Landaux2
1University of the Witwatersrand (Faculty of Health Sciences)
2Centre for Diabetes and Endocrinology (CDE) Johannesburg, South Africa
Abstract
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind randomized placebo-controlled trial.
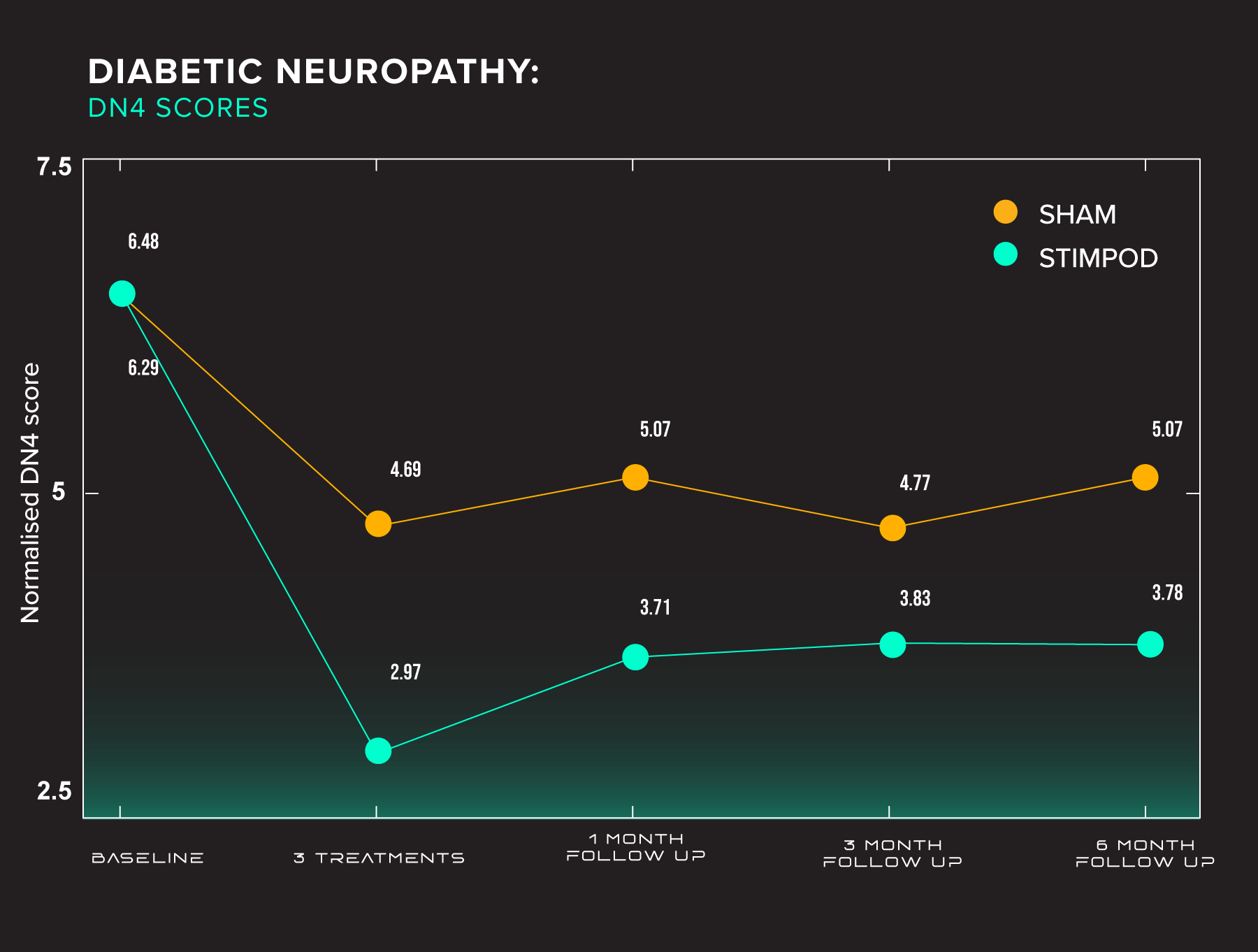
Aim: A randomised single-blind placebo study was conducted on 80 patients with pedal diabetic peripheral neuropathy in 2 cities and their surrounds in South Africa to determine if a pulsed radiofrequency current (PRF) can produce changes in the primary outcome of the DN4 Test and possibly in the BPI-short form.
Method: Patients were selected by their physicians at Centres for Diabetes and randomised into 2 groups – 40 patients each in the groups (A=Active, B =Placebo). Inclusion criteria were pedal Diabetic Peripheral Neuropathy and having a score of 4 or 4+/10 in the DN4 Test. Exclusion criteria: previous experience with the pulsed radiofrequency current and having: peripheral or spinal cord stimulator, pacemaker, metal implants and pregnancy. The DN4 was the primary objective and BPI-SF (secondary) was also tested at baseline, after 3 treatments and 3 follow-ups at 1, 3 and 6 months. Each patient had 3 treatments or a placebo once weekly for 10 mins bilaterally at the sciatic nerve in the popliteal fossa.
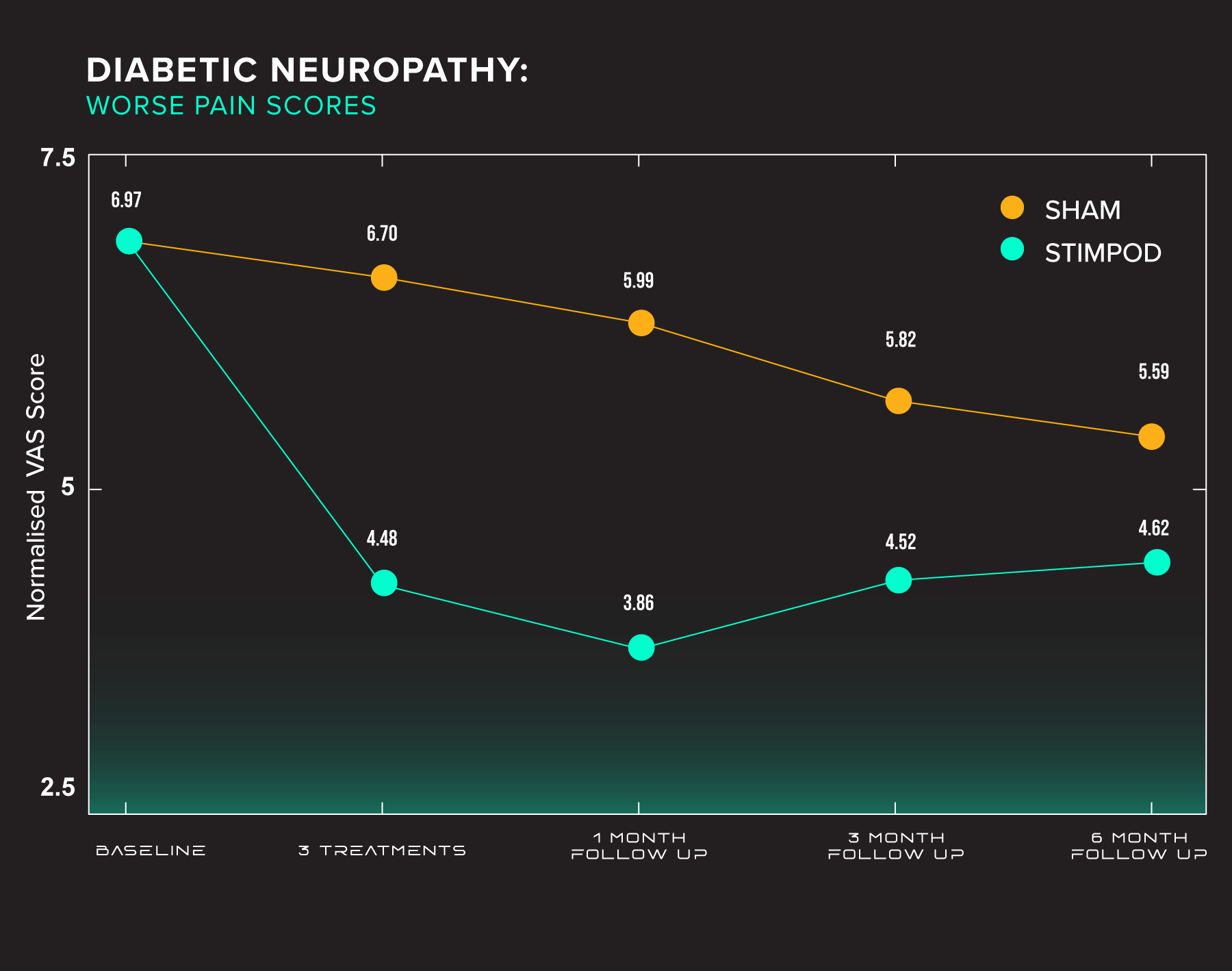
Results: Data were analysed using the SAS version (9.4 statistical program). Results are expressed as mean and standard deviation by groups (A=Active, B=Placebo). There were differences for age and gender in these 2 groups (Age, p=0.030, gender p=0.01) and adjustments were made where applicable. There were also differences evident regardless of age and gender. The DN4 demonstrated that between baseline and 3 treatments there was a reduction in pain and symptoms greater for the A group: p= 0.010 regardless of age and gender. Between baseline and 1 month there was a reduction in pain in both groups, but no significant difference between them p=0.10 but gender and age, nearly significant. There were no differences at 3 and 6 months. In the BPI-SF there were differences between the active and placebo groups in the worst, average and present pain with positive p values some with adjustment for age and gender.
For relations with other people, there was evidence of significant changes some regardless and some adjusted for age and gender and also relations with other people and without analgesics at baseline. There were no differences even after adjustments for age and gender for work and walking ability. None of the BPI-SF variables showed any differences when adjusting for baseline and or analgesics.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Conclusion
After three treatments of PRF current, the DN4 Test demonstrates significant improvements in neuropathic pain and symptoms in certain patients with diabetic peripheral neuropathy.
Pilot Study: Intractable Pain
(Pain Management Centre, Guy’s & St. Thomas’ Hospitals, London UK)
(Pain Management Centre, Guy’s & St. Thomas’ Hospitals, London UK)
External stimulation: simplistic solution to intractable pain
T. Goroszeniuk, S. Kothari
Pain Management Centre, Guy’s & St. Thomas’ Hospitals, London. SE1 7EH. UK
Introduction
Despite adopting a multidisciplinary approach, the management of neuropathic pain not infrequently presents a challenging clinical conundrum. Primary afferent stimulation for the control of chronic pain has been used widely during the last 40 years.
Current locations of access for stimulation include skin in Transcutaneous Electrical Nerve Stimulation (TENS) and acupuncture, peripheral nerve trunks, and primary afferent collaterals in the dorsal columns during Spinal Cord Stimulation (SCS). We have successfully investigated short external low-frequency stimulation either targetted at the site of the maximum pain or deeper afferent sensory nerves in patients with intractable painWe present the preliminary results of our study aimed at symptomatic relief and restoring function in patients with chronic, intractable pain.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Results
We noticed a dramatic reduction of the pain VAS. In 19 cases the VAS reduced to 0 at the end of 5 minutes demonstrating a 100% improvement in their pain status. The VAS scores decreased by 90% in four, 63% in another four and 50% in four more patients. The remaining three cases had their VAS score reduce by 25%, 20% and 15% respectively. In four patients with CRPS, vascular changes were observed at end of the procedure.
Conclusion
External stimulation is a noninvasive, simple and effective initial indicator, in patients with neuropathic pain, prior to longer, medium-term percutaneous stimulating catheter trial and subsequent implantation of permanent devices. The external application component allows the procedure to be performed on an outpatient basis and may be considered for diagnostic and repetitive therapeutic procedures. Further investigation is needed to establish a place for this technique in the management of chronic pain.
References:
- Alo K M., Holsheimer J., New trends in neuromodulation for the management of neuropathic pain. Neurosurgery, 2002, 4,690-704.
- Goroszeniuk T., Goroszeniuk D., Short neuromodulation trial in neuropathic pain produces varying duration but reproducible pain relief. Pain in Europe IV. 4th Congress of EFIC, Prague, 2-6.09.2003.
For decades, electromagnetic therapies have shown clinical effectiveness in treating neurologically-related diseases, wound healing, and bone repair. In this section, we present the clinical trials and pilot studies thus far conducted using Stimpod NMS460 for the treatment of diabetic neuropathies, intractable pain, and migraine.
Clinical Trial: Diabetic Neuropathy
(Randomized, single-blind, placebo-controlled)
(Randomized, single-blind, placebo-controlled)
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind, randomized placebo-controlled trial.
P. Berger1, S. Landaux2
1University of the Witwatersrand (Faculty of Health Sciences)
2Centre for Diabetes and Endocrinology (CDE) Johannesburg, South Africa
Abstract
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind randomized placebo-controlled trial.
Aim: A randomised single-blind placebo study was conducted on 80 patients with pedal diabetic peripheral neuropathy in 2 cities and their surrounds in South Africa to determine if a pulsed radiofrequency current (PRF) can produce changes in the primary outcome of the DN4 Test and possibly in the BPI-short form.
Method: Patients were selected by their physicians at Centres for Diabetes and randomised into 2 groups – 40 patients each in the groups (A=Active, B =Placebo). Inclusion criteria were pedal Diabetic Peripheral Neuropathy and having a score of 4 or 4+/10 in the DN4 Test. Exclusion criteria: previous experience with the pulsed radiofrequency current and having: peripheral or spinal cord stimulator, pacemaker, metal implants and pregnancy. The DN4 was the primary objective and BPI-SF (secondary) was also tested at baseline, after 3 treatments and 3 follow-ups at 1, 3 and 6 months. Each patient had 3 treatments or a placebo once weekly for 10 mins bilaterally at the sciatic nerve in the popliteal fossa.
Results: Data were analysed using the SAS version (9.4 statistical program). Results are expressed as mean and standard deviation by groups (A=Active, B=Placebo). There were differences for age and gender in these 2 groups (Age, p=0.030, gender p=0.01) and adjustments were made where applicable. There were also differences evident regardless of age and gender. The DN4 demonstrated that between baseline and 3 treatments there was a reduction in pain and symptoms greater for the A group: p= 0.010 regardless of age and gender. Between baseline and 1 month there was a reduction in pain in both groups, but no significant difference between them p=0.10 but gender and age, nearly significant. There were no differences at 3 and 6 months. In the BPI-SF there were differences between the active and placebo groups in the worst, average and present pain with positive p values some with adjustment for age and gender.
For relations with other people, there was evidence of significant changes some regardless and some adjusted for age and gender and also relations with other people and without analgesics at baseline. There were no differences even after adjustments for age and gender for work and walking ability. None of the BPI-SF variables showed any differences when adjusting for baseline and or analgesics.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Conclusion
After three treatments of PRF current, the DN4 Test demonstrates significant improvements in neuropathic pain and symptoms in certain patients with diabetic peripheral neuropathy.
Pilot Study: Intractable Pain
(Pain Management Centre, Guy’s & St. Thomas’ Hospitals, London UK)
(Pain Management Centre, Guy’s & St. Thomas’ Hospitals, London UK)
External stimulation: simplistic solution to intractable pain
T. Goroszeniuk, S. Kothari
Pain Management Centre, Guy’s & St. Thomas’ Hospitals, London. SE1 7EH. UK
Introduction
Despite adopting a multidisciplinary approach, the management of neuropathic pain not infrequently presents a challenging clinical conundrum. Primary afferent stimulation for the control of chronic pain has been used widely during the last 40 years.
Current locations of access for stimulation include skin in Transcutaneous Electrical Nerve Stimulation (TENS) and acupuncture, peripheral nerve trunks, and primary afferent collaterals in the dorsal columns during Spinal Cord Stimulation (SCS). We have successfully investigated short external low-frequency stimulation either targetted at the site of the maximum pain or deeper afferent sensory nerves in patients with intractable painWe present the preliminary results of our study aimed at symptomatic relief and restoring function in patients with chronic, intractable pain.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Results
We noticed a dramatic reduction of the pain VAS. In 19 cases the VAS reduced to 0 at the end of 5 minutes demonstrating a 100% improvement in their pain status. The VAS scores decreased by 90% in four, 63% in another four and 50% in four more patients. The remaining three cases had their VAS score reduce by 25%, 20% and 15% respectively. In four patients with CRPS, vascular changes were observed at end of the procedure.
Conclusion
External stimulation is a noninvasive, simple and effective initial indicator, in patients with neuropathic pain, prior to longer, medium-term percutaneous stimulating catheter trial and subsequent implantation of permanent devices. The external application component allows the procedure to be performed on an outpatient basis and may be considered for diagnostic and repetitive therapeutic procedures. Further investigation is needed to establish a place for this technique in the management of chronic pain.
References:
- Alo K M., Holsheimer J., New trends in neuromodulation for the management of neuropathic pain. Neurosurgery, 2002, 4,690-704.
- Goroszeniuk T., Goroszeniuk D., Short neuromodulation trial in neuropathic pain produces varying duration but reproducible pain relief. Pain in Europe IV. 4th Congress of EFIC, Prague, 2-6.09.2003.
Case Reports
![]()
Case Reports
The reports listed in this section has shown such dramatic impact that practitioners using the Stimpod NMS460 felt compelled to share the results with us.
The reports listed in this section has shown such dramatic impact that practitioners using the Stimpod NMS460 felt compelled to share the results with us.