and Case Reports
![]()
White Papers
White Papers
Video introduction to our first white paper
Quantum Biology and Healthcare: the Synergistic Bioeffect of Weak Electromagnetic Fields (EMFs) on Human Bodies
F. Marsili
Research Department, Algiamed Technologies, 2025 Willingdon Avenue #900, Burnaby BC, V5C 0J3, Canada
Abstract
Human bodies are constantly exposed to environmental electromagnetic sources. Both electric and magnetic fields are known to have an active role in altering biological activities. In the present report, the focus will be exclusively on investigating the role of physiological exposure to magnetism. While strong magnetic fields (MFs) are known to induce potentially harmful thermal effects on living systems, there is no existing evidence suggesting possible negative side effects on biological systems from exposure to low-intensity magnetic fields. In recent years, the fast-growing field of quantum biology has focused on characterizing the complex interactions initiated by weak magnetic fields on human bodies through the laws of quantum physics. Even though there is still little understanding of the exact mechanisms, there is sufficient evidence demonstrating short- and long-term physiological changes elicited and, possibly controlled, by magnetic sources. This paper presents a summary of the mechanisms that are potentially, and possibly mutually, involved in eliciting biological reactions to magnetic exposure, supported by experimental evidence. The current understanding of human electromagnetic exposure suggests a potential future role of electromagnetic therapies as non-invasive, effective, and well-tolerated treatments for chronic and acute illnesses.
Podcast: Pathogenesis of Diabetic Neuropathy
Adaptive autonomic and neuroplastic control in diabetic neuropathy: A Narrative Review
C. Birkill, F. Marsili,
P. Potgieter
Research Department, Algiamed Technologies, 2025 Willingdon Avenue #900, Burnaby BC, V5C 0J3, Canada
Abstract
Introduction
Type 2 diabetes mellitus (T2DM) is a worldwide burden to many individuals, as well as to socio-economic and healthcare systems. T2DM is generally accompanied by a variety of metabolic and hemodynamic disorders, as well as nerve dysfunction referred to as diabetic neuropathy (DN). Despite a tremendous body of research, the pathogenesis of DN remains largely elusive.
Currently, two schools of thought exist regarding the pathogenesis of diabetic neuropathy: a) mitochondrial-induced toxicity and neuronal programmed death, and b) microvascular damage and consequent neural degeneration. Both mechanisms signify diabetic neuropathy as an intractable and irreversible disease and, as a consequence, therapeutic approaches focus on treating symptoms with limited efficacy and an elevated risk of side effects.
Methods
This paper, in contrast to current approaches, proposes that the human body exclusively employs mechanisms of adaptation to protect itself during an adverse event. For this purpose, two control systems are defined, namely the autonomic – and the neural control systems, both playing a role in generating distinct adaptive cascades to maintain homeostasis. The autonomic control system responds via inflammatory and immune responses, while the neural control system regulates neural signaling, via plastic adaptation, at both peripheral and central levels. Both systems are proposed to regulate a network of temporal and causative connections which unravel the complex nature of diabetic complications. For example, peripheral neuroplastic events may play a major adaptive role in diabetic neuropathy using restorative mechanisms, similar to what has been explored in brain development and phantom limb syndromes.
Results
A significant result of this approach infers that both autonomic and neuroplastic adaptations make diabetic neuropathies, and other diabetic-related complications, reversible.
Conclusions
In conclusion, the proposed model may open the door to novel therapeutical applications which could trigger the restorative abilities of both the autonomic and neural control.
Video introduction to our first white paper
Quantum Biology and Healthcare: the Synergistic Bioeffect of Weak Electromagnetic Fields (EMFs) on Human Bodies
F. Marsili
Research Department, Algiamed Technologies, 2025 Willingdon Avenue #900, Burnaby BC, V5C 0J3, Canada
Abstract
Human bodies are constantly exposed to environmental electromagnetic sources. Both electric and magnetic fields are known to have an active role in altering biological activities. In the present report, the focus will be exclusively on investigating the role of physiological exposure to magnetism. While strong magnetic fields (MFs) are known to induce potentially harmful thermal effects on living systems, there is no existing evidence suggesting possible negative side effects on biological systems from exposure to low-intensity magnetic fields. In recent years, the fast-growing field of quantum biology has focused on characterizing the complex interactions initiated by weak magnetic fields on human bodies through the laws of quantum physics. Even though there is still little understanding of the exact mechanisms, there is sufficient evidence demonstrating short- and long-term physiological changes elicited and, possibly controlled, by magnetic sources. This paper presents a summary of the mechanisms that are potentially, and possibly mutually, involved in eliciting biological reactions to magnetic exposure, supported by experimental evidence. The current understanding of human electromagnetic exposure suggests a potential future role of electromagnetic therapies as non-invasive, effective, and well-tolerated treatments for chronic and acute illnesses.
Clinical Trials
Clinical Trials
![]()
For decades, electromagnetic therapies have shown clinical effectiveness in treating neurologically-related diseases, wound healing, and bone repair. In this section, we present the clinical trials and pilot studies thus far conducted using Stimpod NMS460 for the treatment of diabetic neuropathies, intractable pain, and migraine.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Long-term, observational study
(India)
Study of the outcome of patients undergoing pulsed radiofrequency for the treatment
of Trigeminal Neuralgia: An observational study.
Neha Sharma, Iqra Nazir Naqash, Zulfiqar Ali, Nadeem Ahmad Khan, Ravouf P Asimi, Imtiyaz A Naqash,
Altaf U Ramzan.
Abstract
Background: Trigeminal neuralgia is chracterised as sudden unilateral severe, stabbing, recurrent episodes of pain in the distribution of one or more branches of
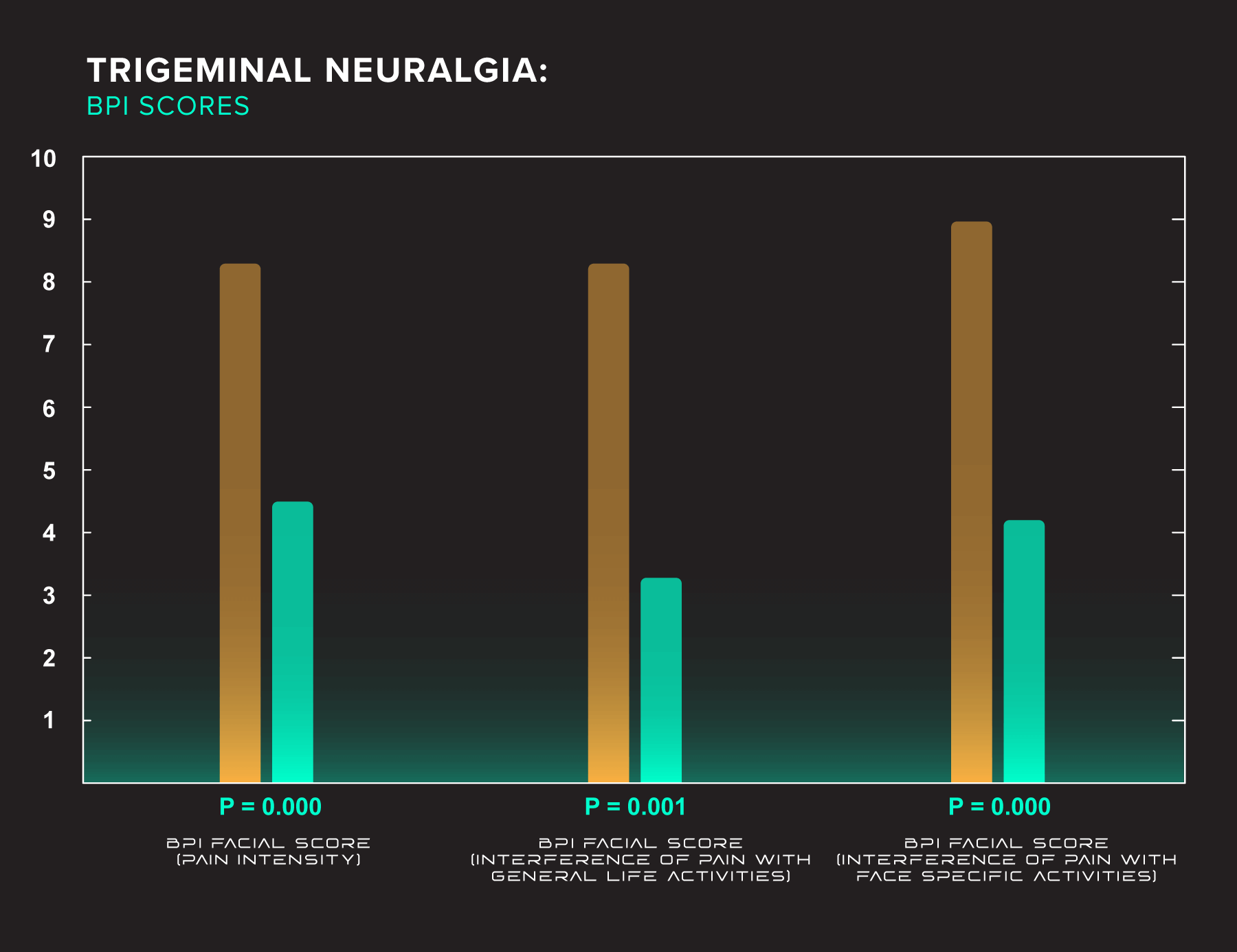
the trigeminal nerve. Pulsed radiofrequency stimulation (PRF) has been recently introduced to alleviate neural, joint pain, and muscle pain. We tried to use PRF for pain relief in trigeminal neuralgia. The primary objective of our study was to observe the effectiveness and safety of pulsed radiofrequency in the patients of trigeminal neuralgia who are refractory to medical management. The secondary objective was to study the effect of pulsed radiofrequency on the duration of pain relief in these patients.
Methodolgy: In this observational study, we enrolled all fresh patients with trigeminal neuralgia attending our pain clinic for the first time and those who had not responded to conservative medical treatment or interventional nerve blocks. All the patients were diagnosed on the basis of signs, symptoms and MRI (CISS sequence). Anatomical landmarks of ophthalarnic nerve, maxillary nerve, mandibular nerve were identified and nerve stimulation was done by placing the probe in the affected nerve division. Each point was stimulated with the radiofrequency probe kept for 10 minutes, giving a current of 10 to 30 milli-amperes with a set frequency of 2 Hertz. A total of 10 settings were given on alternate days. Assessment of pain relief, improvement, or deterioration was done using Barrow Neurological Institute Pain Intensity Score and Brief Pain Inventory facial scale scoring.
Results: There was a significant reduction in pain scores observed on Barrow Neurological Institute (BNI) and Brief Pain Inventory (BPI) pain intensity score (p value of <0.05) before and after pulsed radiofrequency (PRF) application. The duration of pain relief after the application of PRF was up to 180 days in 15 patients, 181-300 days in 8 patients and 300 to 600 days in 7 patients. Only 2 patients had a prolonged pain relief lasting
for 601-720 days. One patient had developed exposure keratitis after 4 sittings of pulsed radiofrequency application at the supraorbital foramen.
Conclusion: PRF offers short term relief in a majority of patients for a period of 18 months to 24 months. However, it was found that the long term effects of PRF may not be seen in patients with TN. PRF may be used as a short term measure for alleviating severe pain of TN till neurolytic
blocks or a definitive surgery is carried out.
Randomized, double-blind, sham-controlled
(India)
Noninvasive neuromodulation of supraorbital and occipital nerves as an adjunct to management of chronic headache
Nazia Tauheed1, Aftab Hussain1, Hira Afzal1, Lubna Zafar2, Hammad Usmani1
1 Department of Anaesthesiology and Critical Care, Jawaharlal Nehru Medical College and Hospital, Aligarh Muslim University, Aligarh, Uttar Pradesh, India
2 Department of Medicine, Jawaharlal Nehru Medical College and Hospital, Aligarh Muslim University, Aligarh, Uttar Pradesh, India
Abstract
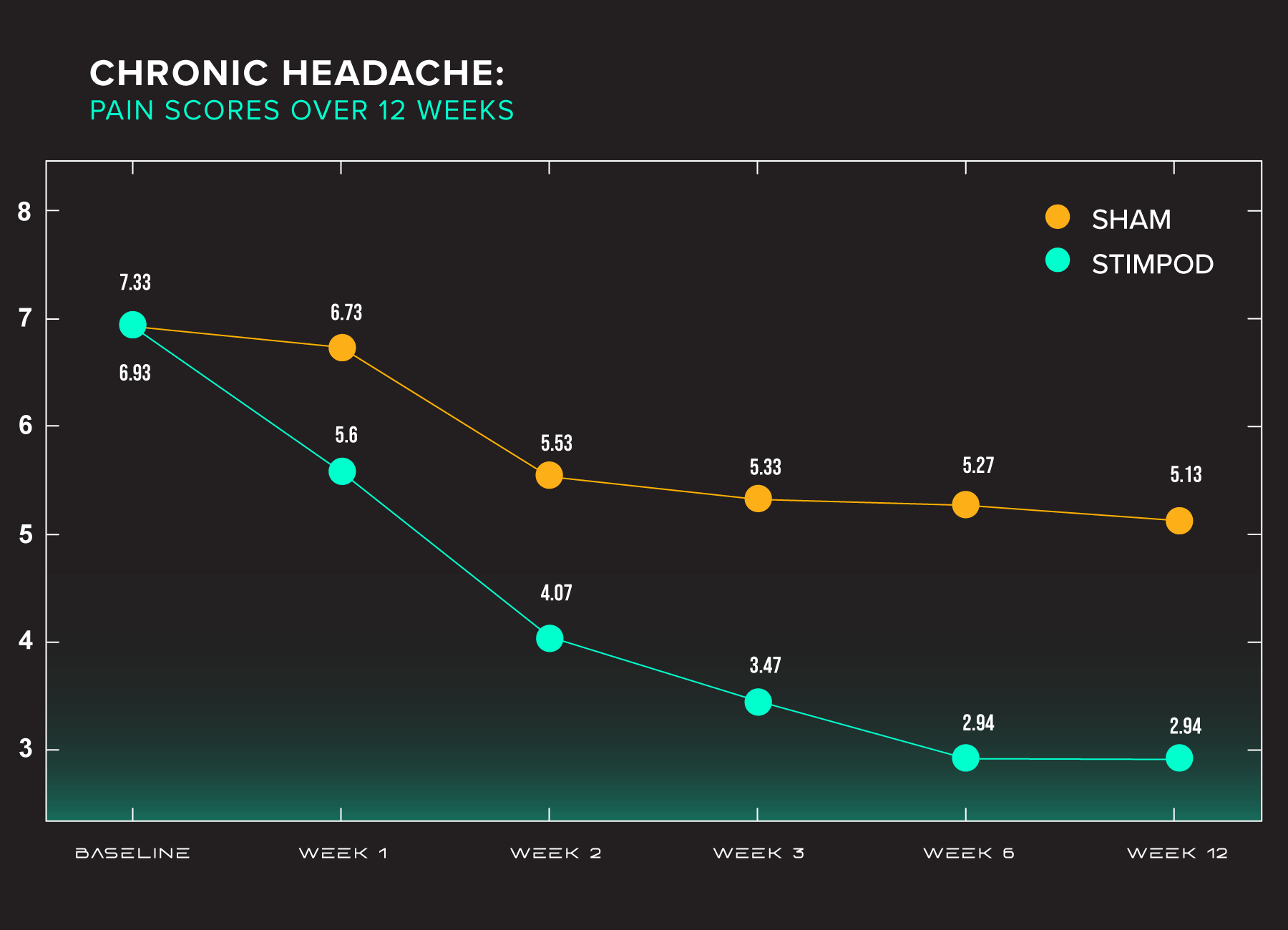
Background: Chronic daily headache (CDH) results in significant distress and a substantial impact on the quality of life. Due to its nature of refractoriness to conservative management, exploring other modalities seems worthwhile. Invasive nerve stimulation, though promising, has seen complication rates in plenty. The goal of the present study was to assess the efficacy of noninvasive neuromodulation of supraorbital and occipital nerves (SON and ON) using hybrid pulsed radiofrequency device (Stimpod NMS460) in patients of CDH.
Methods: Thirty patients suffering from CDH were enrolled in this randomized double‑blind sham‑controlled trial and randomly allocated to two groups of 15 patients each. SON and ON stimulations were given using the device Stimpod NMS460 thrice a week for 3 weeks. Follow‑up visits were scheduled at 6 and 12 weeks of therapy. Pain relief was measured using numerical rating scale score. The overall change in quality of life (measured by Short Form‑12 Health Survey) and associated complications were also noted.
Results: Successful stimulation (50% or greater decrease in pain intensity) was seen in 66.67% patients; inadequate response in 33.3% in the intervention group. The 50% responder rate in sham control group was 13.3%; remaining 86.6% showed an inadequate response. This response remained sustained up to 12 weeks of follow‑up. Similar changes were observed in the quality of life of patients. No adverse effect was documented during the study period.
Conclusion: Noninvasive neuromodulation may serve as a safer and cost‑effective treatment option in CDH refractory to conservative management.
Randomized, single-blind, placebo-controlled
(South Africa)
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind, randomized placebo-controlled trial.
P. Berger1, S. Landaux2
1University of the Witwatersrand (Faculty of Health Sciences)
2Centre for Diabetes and Endocrinology (CDE) Johannesburg, South Africa
Abstract
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind randomized placebo-controlled trial.
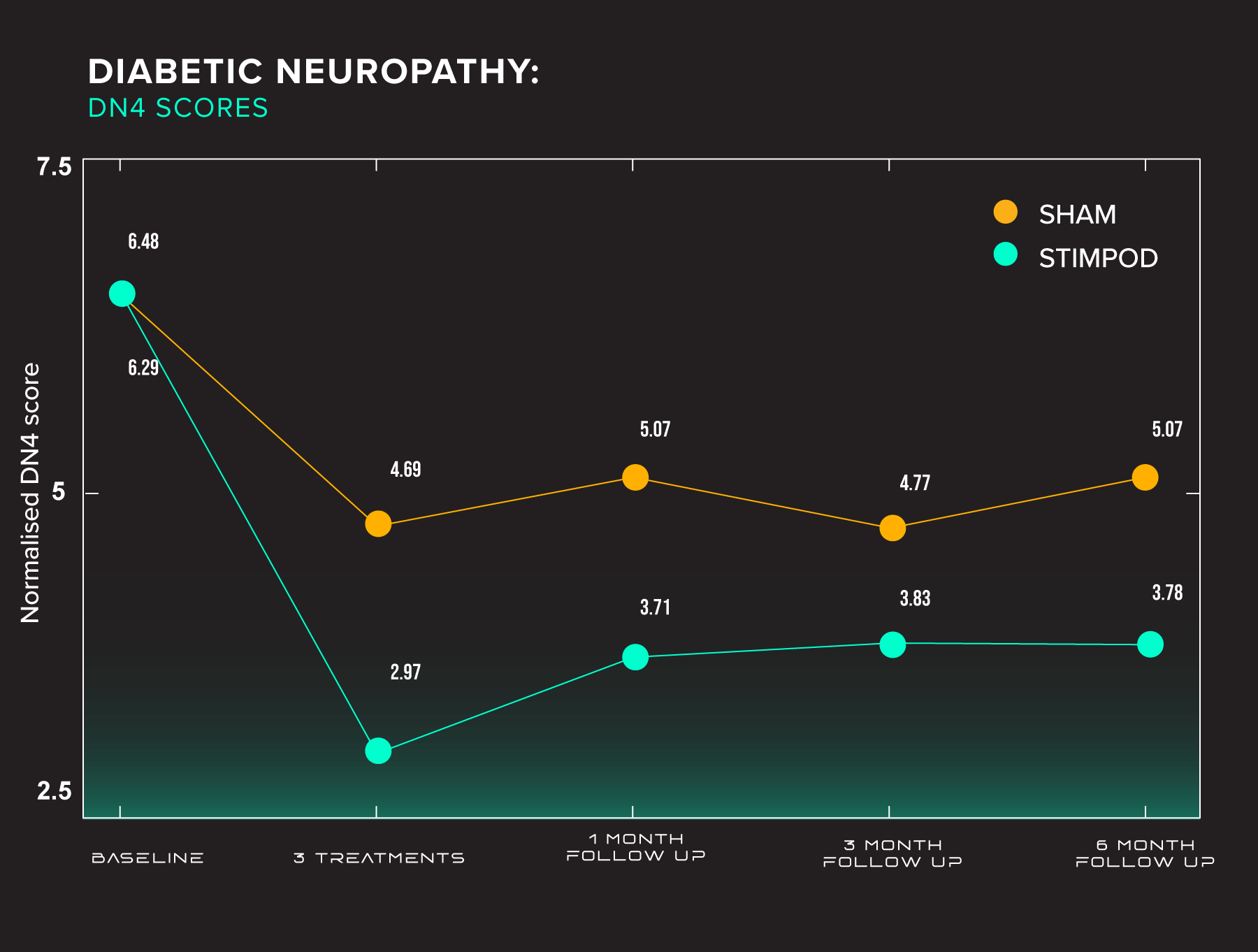
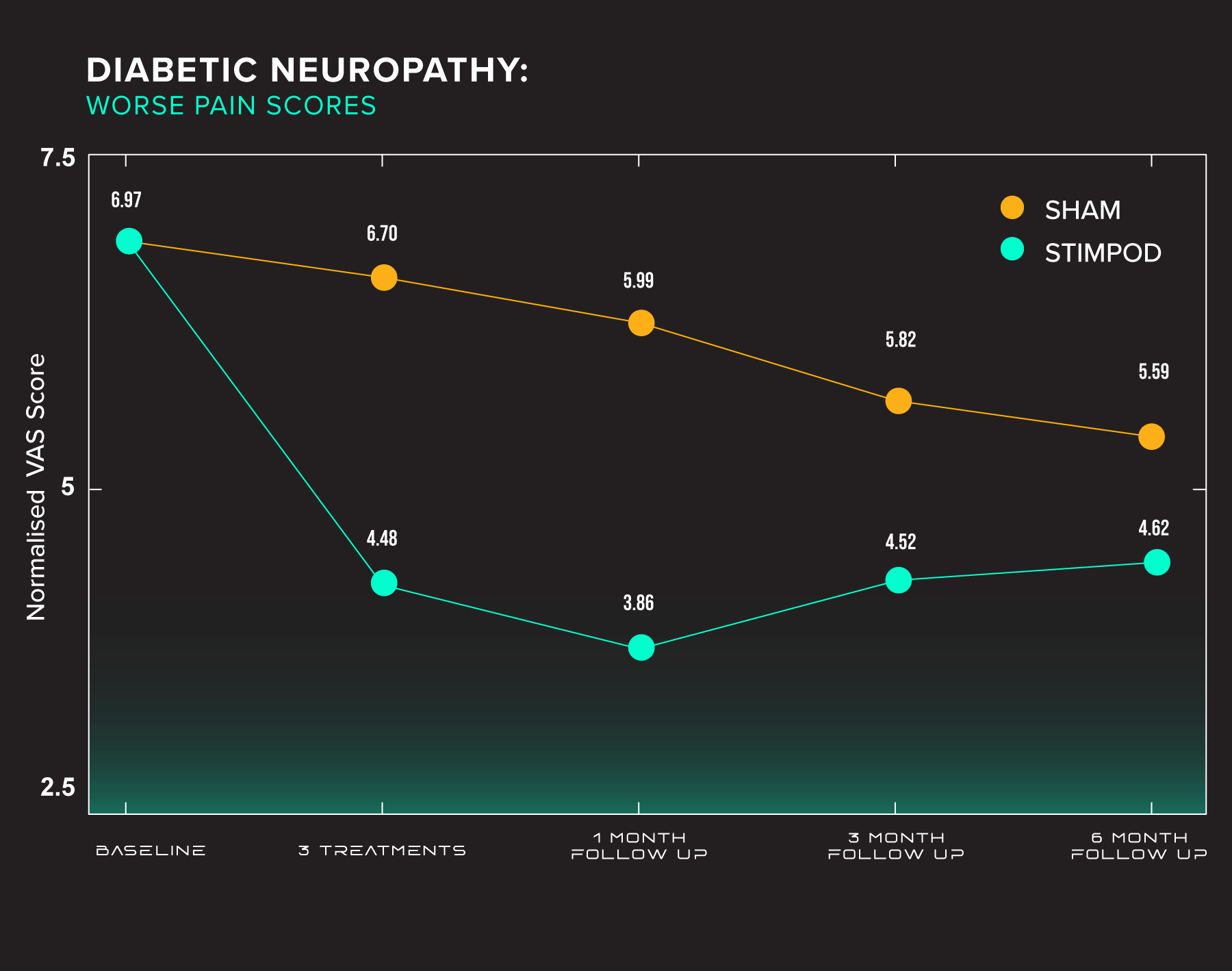
Aim: A randomised single-blind placebo study was conducted on 80 patients with pedal diabetic peripheral neuropathy in 2 cities and their surrounds in South Africa to determine if a pulsed radiofrequency current (PRF) can produce changes in the primary outcome of the DN4 Test and possibly in the BPI-short form.
Method: Patients were selected by their physicians at Centres for Diabetes and randomised into 2 groups – 40 patients each in the groups (A=Active, B =Placebo). Inclusion criteria were pedal Diabetic Peripheral Neuropathy and having a score of 4 or 4+/10 in the DN4 Test. Exclusion criteria: previous experience with the pulsed radiofrequency current and having: peripheral or spinal cord stimulator, pacemaker, metal implants and pregnancy. The DN4 was the primary objective and BPI-SF (secondary) was also tested at baseline, after 3 treatments and 3 follow-ups at 1, 3 and 6 months. Each patient had 3 treatments or a placebo once weekly for 10 mins bilaterally at the sciatic nerve in the popliteal fossa.
Results: Data were analysed using the SAS version (9.4 statistical program). Results are expressed as mean and standard deviation by groups (A=Active, B=Placebo). There were differences for age and gender in these 2 groups (Age, p=0.030, gender p=0.01) and adjustments were made where applicable. There were also differences evident regardless of age and gender. The DN4 demonstrated that between baseline and 3 treatments there was a reduction in pain and symptoms greater for the A group: p= 0.010 regardless of age and gender. Between baseline and 1 month there was a reduction in pain in both groups, but no significant difference between them p=0.10 but gender and age, nearly significant. There were no differences at 3 and 6 months. In the BPI-SF there were differences between the active and placebo groups in the worst, average and present pain with positive p values some with adjustment for age and gender.
For relations with other people, there was evidence of significant changes some regardless and some adjusted for age and gender and also relations with other people and without analgesics at baseline. There were no differences even after adjustments for age and gender for work and walking ability. None of the BPI-SF variables showed any differences when adjusting for baseline and or analgesics.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Conclusion
After three treatments of PRF current, the DN4 Test demonstrates significant improvements in neuropathic pain and symptoms in certain patients with diabetic peripheral neuropathy.
Pain Management Physiotherapy
(South Africa)
Report on a case series investigating a neurostimulation device for the treatment of pain and improvement of mobility and function following elbow surgery
P. Berger, J. Jacks
Pain Management Physiotherapy, Rochester Place, 173 Rivonia Road, Morningside, Johannesburg, South Africa
Introduction
Patients undergoing epicondylitis surgery whether medial or lateral have had chronic elbow pain for a prolonged period often of many months to a year in some cases that has been unresponsive to conservative measures.
Although epicondylitis is a common condition in the arm due to physical overload, the prevalence of definitive lateral epicondylitis was 1.3% and that of medial epicondylitis was 0.4% according to a study in Finland (between 2000 and 2001). The prevalence did not differ between men and women and was highest in subjects aged 45–54 years [1,5]. Prior to surgery these patients have usually had non-surgical treatment and conservative care that includes decreased activity, ice, non-steroidal anti-inflammatory medications, muscle strengthening [2] and these modalities usually help most people. Recalcitrant cases may require cortisone injections that demonstrate the best conservative treatment for lateral epicondylitis [3] but provides only short-term benefits in medial epicondylitis [4]. Lateral epicondylitis, also known as “tennis elbow,” is an overuse syndrome of the common extensor tendon, predominantly affecting the extensor carpi radialis brevis. Patients complain of poorly defined pain located over the lateral elbow that is typically exacerbated by activities requiring wrist extension and/or wrist supination against resistance. There will often be pain in the morning as well as after any period of time that the elbow has been held in a flexed position [5]. Medial epicondylitis is a clinical entity characterized by pain in the medial aspect of the elbow and dysfunction induced by degenerative changes in the origin of the flexor–pronator muscle mass.The accumulated pathological evidence suggests that the process is associated with fibrillary degeneration of collagen and angiofibroblastic hyperplasia at the origin of the flexor pronator muscle mass, microfragmentation or tears of the tendon, accumulation of vascular granulation tissue and tendinous necrosis, all of which are also accompanied by a secondary inflammatory reaction [6]. Non-operative treatment has been deemed highly successful,yet the few prospective reports available suggest that symptoms frequently persist or recur. Operative treatment is indicated for debilitating pain that is diagnosed after the exclusion of other pathologic causes for pain and that persists in spite of a well-managed non-operative regimen spanning a minimum of 6 months. The surgical technique involves excision of the pathologic portion of the tendon, repair of the resulting defect, and reattachment of the origin to the lateral or medial epicondyle.
Surgical treatment results in a high degree of subjective relief, although objective strength deficits may persist [7]. During the last decade, increased attention has been paid to persistent pain complaints after almost any surgical operation with reported incidences ranging between 5% and 50% [8]. The International Association for the Study of Pain defines post-surgical pain as persistent pain after surgery of greater than three months duration[9]. Persistent post-surgical pain syndromes (PPSP) have been considered neuropathic [8] and a strong association is reported between PPSP and sensory abnormalities [10]; however, there is evidence that mechanisms other than nerve injury such as inflammation, central sensitization or a combination of these may play a role. It is important to elucidate whether persistent pain is due to surgical injury of the nerves, ongoing inflammatory processes,injury to the somatic or visceral structures or other causes [11]. Most of those patients that elected to have the surgery for the elbow in these case reports had chronic pain before surgery with or without neuropathic symptoms. It was thought that treating the acute post-operative pain aggressively early by blocking pain,improving wound healing and improving strength may have some impact on post-surgical pain.
Methods
Seven patients who had elbow surgery either for golfers or tennis elbow were sent for neurostimulation within a day post-surgery. The University of the Witwatersrand Human Ethics Committee approval was received for the study. An information and consent form was presented to patients and duly signed.
The treatment protocol was divided into two sections.
The first three treatments with non-invasive pulsed radio frequency:
- 20 min in total
- brachial plexus region for 10 min superior to the clavicle
- brachial plexus region for 10 min inferior to the clavicle
This treatment was given on alternate days over 1 week before the splint was removed and the aim was to reduce pain immediately and to have a possible influence on post-operative pain syndromes that may occur, to prime the nerve supply to the elbow to increase mobility and to improve muscle strength (this could be visualized by fasciculation of the muscles under the splint) to enable better function after the splint was removed.
Once the splint was removed all measures and evaluations were taken before the second section of treatment was implemented.
Results
In the patient study group there were four females and three males and the ages ranged from 38 to 60 years. Only one patient had a golfers elbow repair the remainder had a tennis elbow repair. Five patients recovered well and two patients had to have the surgery redone due in the first patient to a complication within the arm due to a previous knife wound and a more extensive approach being required than as in the initial surgery and in the other patient re-operation was required after a fall that had occurred during the recovery period damaging the original site of the surgery.
There was significant pain post-surgery but the movements of flexion and extension were already quite advanced immediately after the splint was removed and this may have been expedited by the electrical stimulation. There were only two movements such as making a fist and washing the face that were evaluated on the fourth treatment as all others were not attainable and there were 12 movements that were attainable and evaluated from the sixth to ninth treatment.
Patient 107 had a good range of movement of flexion and patient 102 had a good range of extension before the 4th treatment.
On the last treatment, pain levels were greatly reduced except for the patient that had to be re-operated. Range of movements and activities were achieved or almost full.
Conclusion
Prior to this case series of patients undergoing epicondylitis surgery the author had evaluated a random group of eight patients from 2006 to 2011 from the patient records that had also had the above mentioned surgery and had been referred by their orthopaedic surgeons for pain control and improved mobility.
On evaluation of this group of patients there was consistency with other studies in the comparison of their ages, gender and type of surgery with lateral epicondylitis surgery performed more frequently that medial epicondylitis surgery [1,5]. Unfortunately there was limited information in VAS and wound status in some of the patients but there was evidence of some patients requiring treatment many weeks after surgery, 16 weeks in one patient with the minimum referral being 10 days after surgery. There were a minimum number of treatments provided in one patient of two treatments and a maximum number of 12 treatments in another patient, with varying numbers of treatments in the others. Some of the wounds were oedematous and inflamed, most of the patients had limitation of extension of the elbow and there was only 50% resolution of the condition in these elbows according to the notes scrutinized. The treatments that were offered to these patients were usually multiple modalities that included ultrasound, electro-acupuncture, infrared laser, functional electrical stimulation, stretching, mobilization of the joint and exercises depending on the condition. These treatments would extend for longer than 20 min duration.
Although the incidence of neuropathic pain and or PPSP in elbow surgery is minimal yet chronic pain may be more common than realized. The condition could elicit chronic pain that may be due to pathogenic mechanisms that can be ascribed to preoperative, intra-operative and post-operative factors and that may produce ongoing complications for the patient and even neuropathic symp-toms. It was then decided to use this example of post-operative elbow surgery for treatment with a neurostimulator (Stimpod) that is minimal, non-invasive, of short duration and cost-effective and may prevent PPSP and relieve neuropathic symptoms.
In the results achieved the patients in the pilot study had some relief of severe and uncomfortable pain before the splint was removed and they required less medication than prescribed as it was given on an as needed basis. After the splint was removed pain levels increased as mobility improved but the pain increase was due to stretching of injured tissues with active movements and did not produce chronic and or spontaneous pain.
The most surprising effect was the movement that was already available immediately after the splint was removed and that continued to improve to full range without the usual treatment requiring mobilization, stretching and strengthening during rehabilitation.
The wounds also demonstrated minimal oedema and inflamma-tion that is not usually expected with recent surgery and continued to improve in some cases to an imperceptible scar. Scarring and sen-sitivity in the wound may augur chronic pain conditions and it is imperative to block pain and improve wound healing to prevent persistent pain and dysfunction.
By the last treatment patients had significantly improved and at one month after the last treatment the patients had almost all attained their goals of pain relief, range of movement and strength in their functional activities.
Patients were generally content with their progress in pain, movement and the type of treatment that was offered as it was of short duration, with a limited number of treatments required to achieve these results with minimal discomfort.
The neurostimulation device stimulated the brachial plexus in the first three treatments that then activates the specific nerve sup-ply affected by the operation, e.g. radial nerve superior and inferior to the elbow if a lateral epicodylitis surgery was performed. Initially this stimulation produced minimal fasciculation in the nerve but as the nerve conduction improved then activity within the nerve sup-ply became more evident with strong fasciculations occurring. This current could also translate in the opposite direction to the dorsal root ganglion of the cervical nerve roots.
When the splint was removed and the wound was exposed the neurostimulation was then applied to the radial nerve (in lateral epicondylitis surgery) superior and inferior to the elbow and to either end of the wound. The effect of this was increased fasciculations in the radial nerve and this even occurred with stimulation on the wound. Again the current would translate in the opposite direction to the brachial plexus and the dorsal root ganglion of the nerve involved.
The neurostimulation device that has been used in this case series appears to have effects on nerve conduction e.g. found in Bell’s palsy patients and relieves neuropathic pain from different aetiologies in many clinical situations since 2009 [12,20].
This type of neurostimulation was originally developed from a nerve-mapping device used by anaesthetists (2003) to detect a nerve before injecting and creating a nerve block prior to surgery. It was thought that to apply a magnetic field of 133 kHz to the square wave component of the nerve mapping current, a treatment would be developed that may be similar to that used in conventional pulsed radiofrequency (PRF) and that also included nerve mapping detection. In effect the current can target the nerve supply to an injury or damaged region. It is possible that nerve stimulation of the affected nerve may become a seminal treatment for blocking pain, normalizing nerve conduction with improvement in strength and range of movements. This treatment would there-fore be non-invasive and of short duration to create these healing effects.
In conventional PRF there is no destruction of the tissue involved (this could be at the dorsal root ganglion, among others) and it is the presence of the high frequency (pulsed 500 kHz) that improves nerve pain and dysfunction, albeit during an invasive procedure. It is also known that pulsed and continuous radio frequency adjacent to the dorsal root ganglion in a rat model induces latent cellular activity [22]. Neuroscientists measure expression of c-fos as an indirect marker of neuronal activity as c-fos is often expressed when neurons fire action potentials. Up-regulation of c-fos mRNA in a neuron indicates recent activity [23].
The neurostimulation provided to these patients demonstrated a capacity to decrease acute post-surgical pain, improve mobility and wound healing with treatment of short duration and minimal intervention by the physiotherapist. There was no sign of neuropathic symptoms in these patients 6 months post-surgery and any pain that was experienced could be attributed to a normal post-operative healing process and improvement in strength with functional activities. All patients were able to resume their normal function and sporting activities.
References:
- Shiri R, Vilkari-Juntura E, Varonen H, Heliovaara M. Prevalance and determinants of lateral and medial epicondylitis: a population study. Am J Epidemiol 2006;164(11):1065–74.
- Leach RE, Miller JK. Lateral and medical condylitis of the elbow. Clin Sports Med 1987;6(2):259–72.
- Tonks JH, Pai SK, Murali SR. Steroid injection therapy is the best conservative treatment for lateral epicondylitis: a prospective randomized controlled trial. Int J Clin Pract 2007;61(2):240–6.
- Stahl S, Kaufman T. The efficacy of an injection of steroids for medial epicondylitis. A prospective study of 60 elbows. J Bone joint Surg AM 1997;79(11):1648–52.
- Levin D, Levon NN, Miller TT, O’Kane PL, Feld RI, Parker L, et al. Lateral epicondylitis of the elbow: US findings. Radiology 2005;237(1), http://dx.doi.org/10.1148/radiol.2371040784.
- Bennet JB. Lateral and medial epicondylitis. Hand Clinic 1994;10:157–63.
- Jobe FW, Ciccotti MG. Lateral and medial epicondylitis of the elbow. J Am Acad Orthop Surg 1994;2(1):1–8.
- Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet 2006;367:1618–25.
- Poobalan AS, Bruce J, Smith W, Cairns S, King PM, Krukowski ZH, et al. A review of chronic pain after inguinal herniorrhaphy. Clin J Pain 2003;19(1):48–54.
- Kairaluroma PM, Bachmann MS, Rosenberg PH, Pere PJ. Preincisional paraverte-bral block reduces the prevalence of chronic pain after breast surgery. Anaesth Analg 2006;103:703–8.
- Haroutiunian S, Nikolajsen L, Finnerup NB, Jensen TS. The neuropathic com-ponent in persistent postsurgical pain: a systematic literature review. Pain 2013;154:95–102.
- Berger P. Electrical current and acupuncture treatment for a paediatric patient with a recurring long thoracic nerve paralysis. Acupunct Relat Ther 2014;2:14–8.
- Woolf CJ, Chong M-S. Preemptive analgesia-treating postoperative pain by preventing the establishment of central sensitization. Anaesth Analg 1993;77(2):362–79.
- Johansen A, Romundstad L, Nielsen CS, Schirmer H, Stubhaug A. Persistent postsurgical pain in the general population: prevalence and predictors in the Trompso study. Pain 2012;153:1390–6.
- Dualec C, Guastella V, Morand D, Cardot JM, Aublet-Cuvelier B, Mulliez A, et al. Characteristics of the neuropathy induced by thoracotomy: a 4-month follow-up study with psychophysical examination. Clin J Pain 2011;27:471–80.
- Bjordal JM, Johnson MJ, Ljunggreen L. Transcutaneous electrical nerve stimula-tion can reduce post-operative analgesic consumption in a meta-analysis with assessment of optimal treatment parameters for postoperative pain. Eur J Pain 2012;7:181–8.
- Johnson M. Transcutaneous electrical nerve stimulation; 2012, http://dx.doi.org/10.1002/9780470015902.a0024044 [Published online].
- Freynet A, Falcoz P-E. Control of post-thoracotomy pain by transcutaneous electrical nerve stimulation: effect on serum cytokine levels, visual ana-logue scale, pulmonary function and medication. Eur J Cardiothorac Surg 2012;41(4):861–8.
- Benedetti F, Amanzio M, Casadio C, Cavallo A, Cianci R, Giobbe R, et al. Con-trol of postoperative pain by transcutaneous electrical nerve stimulation after thoracic operations. Ann Thorac Surg 1997;63(3):773–6.
- Berger P. Intro NMS 460: a non-invasive pulsed radio frequency current for pain relief and nerve degeneration. Pretoria, South Africa: Xavant Technology; 2012.
- Vodovnik L, Karba R. Treatment of chronic wounds by means of electric and electromagnetic fields. Part 1. Literature review. Med Biol Eng Comput 1992;30:257–68.
- Van Zundert J, de Louw AJA, Joosten EAJ, Kessels AGH, Honig W, Dederen PJ, et al. Pulsed and continuous radio frequency adjacent to the dorsal root ganglion of rat induces latent cellular activity. Anesthesiology 2005;102(1):125–31.
- Dragunow M, Faull R. The use of c-fos as a metabolic marker in neuronal path-way tracing. J Neurosci Methods 1989;29(3):261–5.
Pain Management Centre, Guy’s & St. Thomas’ Hospitals
(United Kingdom)
External stimulation: simplistic solution to intractable pain
T. Goroszeniuk, S. Kothari
Pain Management Centre, Guy’s & St. Thomas’ Hospitals, London. SE1 7EH. UK
Introduction
Despite adopting a multidisciplinary approach, the management of neuropathic pain not infrequently presents a challenging clinical conundrum. Primary afferent stimulation for the control of chronic pain has been used widely during the last 40 years.
Current locations of access for stimulation include skin in Transcutaneous Electrical Nerve Stimulation (TENS) and acupuncture, peripheral nerve trunks, and primary afferent collaterals in the dorsal columns during Spinal Cord Stimulation (SCS). We have successfully investigated short external low-frequency stimulation either targetted at the site of the maximum pain or deeper afferent sensory nerves in patients with intractable painWe present the preliminary results of our study aimed at symptomatic relief and restoring function in patients with chronic, intractable pain.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Results
We noticed a dramatic reduction of the pain VAS. In 19 cases the VAS reduced to 0 at the end of 5 minutes demonstrating a 100% improvement in their pain status. The VAS scores decreased by 90% in four, 63% in another four and 50% in four more patients. The remaining three cases had their VAS score reduce by 25%, 20% and 15% respectively. In four patients with CRPS, vascular changes were observed at end of the procedure.
Conclusion
External stimulation is a noninvasive, simple and effective initial indicator, in patients with neuropathic pain, prior to longer, medium-term percutaneous stimulating catheter trial and subsequent implantation of permanent devices. The external application component allows the procedure to be performed on an outpatient basis and may be considered for diagnostic and repetitive therapeutic procedures. Further investigation is needed to establish a place for this technique in the management of chronic pain.
References:
- Alo K M., Holsheimer J., New trends in neuromodulation for the management of neuropathic pain. Neurosurgery, 2002, 4,690-704.
- Goroszeniuk T., Goroszeniuk D., Short neuromodulation trial in neuropathic pain produces varying duration but reproducible pain relief. Pain in Europe IV. 4th Congress of EFIC, Prague, 2-6.09.2003.
For decades, electromagnetic therapies have shown clinical effectiveness in treating neurologically-related diseases, wound healing, and bone repair. In this section, we present the clinical trials and pilot studies thus far conducted using Stimpod NMS460 for the treatment of diabetic neuropathies, intractable pain, and migraine.
Long-term, observational study
(India)
Study of the outcome of patients undergoing pulsed radiofrequency for the treatment
of Trigeminal Neuralgia: An observational study.
Neha Sharma, Iqra Nazir Naqash, Zulfiqar Ali, Nadeem Ahmad Khan, Ravouf P Asimi, Imtiyaz A Naqash,
Altaf U Ramzan.
Abstract
Background: Trigeminal neuralgia is chracterised as sudden unilateral severe, stabbing, recurrent episodes of pain in the distribution of one or more branches of
the trigeminal nerve. Pulsed radiofrequency stimulation (PRF) has been recently introduced to alleviate neural, joint pain, and muscle pain. We tried to use PRF for pain relief in trigeminal neuralgia. The primary objective of our study was to observe the effectiveness and safety of pulsed radiofrequency in the patients of trigeminal neuralgia who are refractory to medical management. The secondary objective was to study the effect of pulsed radiofrequency on the duration of pain relief in these patients.
Methodolgy: In this observational study, we enrolled all fresh patients with trigeminal neuralgia attending our pain clinic for the first time and those who had not responded to conservative medical treatment or interventional nerve blocks. All the patients were diagnosed on the basis of signs, symptoms and MRI (CISS sequence). Anatomical landmarks of ophthalarnic nerve, maxillary nerve, mandibular nerve were identified and nerve stimulation was done by placing the probe in the affected nerve division. Each point was stimulated with the radiofrequency probe kept for 10 minutes, giving a current of 10 to 30 milli-amperes with a set frequency of 2 Hertz. A total of 10 settings were given on alternate days. Assessment of pain relief, improvement, or deterioration was done using Barrow Neurological Institute Pain Intensity Score and Brief Pain Inventory facial scale scoring.
Results: There was a significant reduction in pain scores observed on Barrow Neurological Institute (BNI) and Brief Pain Inventory (BPI) pain intensity score (p value of <0.05) before and after pulsed radiofrequency (PRF) application. The duration of pain relief after the application of PRF was up to 180 days in 15 patients, 181-300 days in 8 patients and 300 to 600 days in 7 patients. Only 2 patients had a prolonged pain relief lasting
for 601-720 days. One patient had developed exposure keratitis after 4 sittings of pulsed radiofrequency application at the supraorbital foramen.
Conclusion: PRF offers short term relief in a majority of patients for a period of 18 months to 24 months. However, it was found that the long term effects of PRF may not be seen in patients with TN. PRF may be used as a short term measure for alleviating severe pain of TN till neurolytic
blocks or a definitive surgery is carried out.
Randomized, double-blind, sham-controlled
(India)
Noninvasive neuromodulation of supraorbital and occipital nerves as an adjunct to management of chronic headache
Nazia Tauheed1, Aftab Hussain1, Hira Afzal1, Lubna Zafar2, Hammad Usmani1
1 Department of Anaesthesiology and Critical Care, Jawaharlal Nehru Medical College and Hospital, Aligarh Muslim University, Aligarh, Uttar Pradesh, India
2 Department of Medicine, Jawaharlal Nehru Medical College and Hospital, Aligarh Muslim University, Aligarh, Uttar Pradesh, India
Abstract
Background: Chronic daily headache (CDH) results in significant distress and a substantial impact on the quality of life. Due to its nature of refractoriness to conservative management, exploring other modalities seems worthwhile. Invasive nerve stimulation, though promising, has seen complication rates in plenty. The goal of the present study was to assess the efficacy of noninvasive neuromodulation of supraorbital and occipital nerves (SON and ON) using hybrid pulsed radiofrequency device (Stimpod NMS460) in patients of CDH.
Methods: Thirty patients suffering from CDH were enrolled in this randomized double‑blind sham‑controlled trial and randomly allocated to two groups of 15 patients each. SON and ON stimulations were given using the device Stimpod NMS460 thrice a week for 3 weeks. Follow‑up visits were scheduled at 6 and 12 weeks of therapy. Pain relief was measured using numerical rating scale score. The overall change in quality of life (measured by Short Form‑12 Health Survey) and associated complications were also noted.
Results: Successful stimulation (50% or greater decrease in pain intensity) was seen in 66.67% patients; inadequate response in 33.3% in the intervention group. The 50% responder rate in sham control group was 13.3%; remaining 86.6% showed an inadequate response. This response remained sustained up to 12 weeks of follow‑up. Similar changes were observed in the quality of life of patients. No adverse effect was documented during the study period.
Conclusion: Noninvasive neuromodulation may serve as a safer and cost‑effective treatment option in CDH refractory to conservative management.
Randomized, single-blind, placebo-controlled
(South Africa)
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind, randomized placebo-controlled trial.
P. Berger1, S. Landaux2
1University of the Witwatersrand (Faculty of Health Sciences)
2Centre for Diabetes and Endocrinology (CDE) Johannesburg, South Africa
Abstract
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind randomized placebo-controlled trial.
Aim: A randomised single-blind placebo study was conducted on 80 patients with pedal diabetic peripheral neuropathy in 2 cities and their surrounds in South Africa to determine if a pulsed radiofrequency current (PRF) can produce changes in the primary outcome of the DN4 Test and possibly in the BPI-short form.
Method: Patients were selected by their physicians at Centres for Diabetes and randomised into 2 groups – 40 patients each in the groups (A=Active, B =Placebo). Inclusion criteria were pedal Diabetic Peripheral Neuropathy and having a score of 4 or 4+/10 in the DN4 Test. Exclusion criteria: previous experience with the pulsed radiofrequency current and having: peripheral or spinal cord stimulator, pacemaker, metal implants and pregnancy. The DN4 was the primary objective and BPI-SF (secondary) was also tested at baseline, after 3 treatments and 3 follow-ups at 1, 3 and 6 months. Each patient had 3 treatments or a placebo once weekly for 10 mins bilaterally at the sciatic nerve in the popliteal fossa.
Results: Data were analysed using the SAS version (9.4 statistical program). Results are expressed as mean and standard deviation by groups (A=Active, B=Placebo). There were differences for age and gender in these 2 groups (Age, p=0.030, gender p=0.01) and adjustments were made where applicable. There were also differences evident regardless of age and gender. The DN4 demonstrated that between baseline and 3 treatments there was a reduction in pain and symptoms greater for the A group: p= 0.010 regardless of age and gender. Between baseline and 1 month there was a reduction in pain in both groups, but no significant difference between them p=0.10 but gender and age, nearly significant. There were no differences at 3 and 6 months. In the BPI-SF there were differences between the active and placebo groups in the worst, average and present pain with positive p values some with adjustment for age and gender.
For relations with other people, there was evidence of significant changes some regardless and some adjusted for age and gender and also relations with other people and without analgesics at baseline. There were no differences even after adjustments for age and gender for work and walking ability. None of the BPI-SF variables showed any differences when adjusting for baseline and or analgesics.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Conclusion
After three treatments of PRF current, the DN4 Test demonstrates significant improvements in neuropathic pain and symptoms in certain patients with diabetic peripheral neuropathy.
Pain Management Physiotherapy
(South Africa)
Report on a case series investigating a neurostimulation device for the treatment of pain and improvement of mobility and function following elbow surgery
P. Berger, J. Jacks
Pain Management Physiotherapy, Rochester Place, 173 Rivonia Road, Morningside, Johannesburg, South Africa
Introduction
Patients undergoing epicondylitis surgery whether medial or lateral have had chronic elbow pain for a prolonged period often of many months to a year in some cases that has been unresponsive to conservative measures.
Although epicondylitis is a common condition in the arm due to physical overload, the prevalence of definitive lateral epicondylitis was 1.3% and that of medial epicondylitis was 0.4% according to a study in Finland (between 2000 and 2001). The prevalence did not differ between men and women and was highest in subjects aged 45–54 years [1,5]. Prior to surgery these patients have usually had non-surgical treatment and conservative care that includes decreased activity, ice, non-steroidal anti-inflammatory medications, muscle strengthening [2] and these modalities usually help most people. Recalcitrant cases may require cortisone injections that demonstrate the best conservative treatment for lateral epicondylitis [3] but provides only short-term benefits in medial epicondylitis [4]. Lateral epicondylitis, also known as “tennis elbow,” is an overuse syndrome of the common extensor tendon, predominantly affecting the extensor carpi radialis brevis. Patients complain of poorly defined pain located over the lateral elbow that is typically exacerbated by activities requiring wrist extension and/or wrist supination against resistance. There will often be pain in the morning as well as after any period of time that the elbow has been held in a flexed position [5]. Medial epicondylitis is a clinical entity characterized by pain in the medial aspect of the elbow and dysfunction induced by degenerative changes in the origin of the flexor–pronator muscle mass.The accumulated pathological evidence suggests that the process is associated with fibrillary degeneration of collagen and angiofibroblastic hyperplasia at the origin of the flexor pronator muscle mass, microfragmentation or tears of the tendon, accumulation of vascular granulation tissue and tendinous necrosis, all of which are also accompanied by a secondary inflammatory reaction [6]. Non-operative treatment has been deemed highly successful,yet the few prospective reports available suggest that symptoms frequently persist or recur. Operative treatment is indicated for debilitating pain that is diagnosed after the exclusion of other pathologic causes for pain and that persists in spite of a well-managed non-operative regimen spanning a minimum of 6 months. The surgical technique involves excision of the pathologic portion of the tendon, repair of the resulting defect, and reattachment of the origin to the lateral or medial epicondyle.
Surgical treatment results in a high degree of subjective relief, although objective strength deficits may persist [7]. During the last decade, increased attention has been paid to persistent pain complaints after almost any surgical operation with reported incidences ranging between 5% and 50% [8]. The International Association for the Study of Pain defines post-surgical pain as persistent pain after surgery of greater than three months duration[9]. Persistent post-surgical pain syndromes (PPSP) have been considered neuropathic [8] and a strong association is reported between PPSP and sensory abnormalities [10]; however, there is evidence that mechanisms other than nerve injury such as inflammation, central sensitization or a combination of these may play a role. It is important to elucidate whether persistent pain is due to surgical injury of the nerves, ongoing inflammatory processes,injury to the somatic or visceral structures or other causes [11]. Most of those patients that elected to have the surgery for the elbow in these case reports had chronic pain before surgery with or without neuropathic symptoms. It was thought that treating the acute post-operative pain aggressively early by blocking pain,improving wound healing and improving strength may have some impact on post-surgical pain.
Methods
Seven patients who had elbow surgery either for golfers or tennis elbow were sent for neurostimulation within a day post-surgery. The University of the Witwatersrand Human Ethics Committee approval was received for the study. An information and consent form was presented to patients and duly signed.
The treatment protocol was divided into two sections.
The first three treatments with non-invasive pulsed radio frequency:
- 20 min in total
- brachial plexus region for 10 min superior to the clavicle
- brachial plexus region for 10 min inferior to the clavicle
This treatment was given on alternate days over 1 week before the splint was removed and the aim was to reduce pain immediately and to have a possible influence on post-operative pain syndromes that may occur, to prime the nerve supply to the elbow to increase mobility and to improve muscle strength (this could be visualized by fasciculation of the muscles under the splint) to enable better function after the splint was removed.
Once the splint was removed all measures and evaluations were taken before the second section of treatment was implemented.
Results
In the patient study group there were four females and three males and the ages ranged from 38 to 60 years. Only one patient had a golfers elbow repair the remainder had a tennis elbow repair. Five patients recovered well and two patients had to have the surgery redone due in the first patient to a complication within the arm due to a previous knife wound and a more extensive approach being required than as in the initial surgery and in the other patient re-operation was required after a fall that had occurred during the recovery period damaging the original site of the surgery.
There was significant pain post-surgery but the movements of flexion and extension were already quite advanced immediately after the splint was removed and this may have been expedited by the electrical stimulation. There were only two movements such as making a fist and washing the face that were evaluated on the fourth treatment as all others were not attainable and there were 12 movements that were attainable and evaluated from the sixth to ninth treatment.
Patient 107 had a good range of movement of flexion and patient 102 had a good range of extension before the 4th treatment.
On the last treatment, pain levels were greatly reduced except for the patient that had to be re-operated. Range of movements and activities were achieved or almost full.
Conclusion
Prior to this case series of patients undergoing epicondylitis surgery the author had evaluated a random group of eight patients from 2006 to 2011 from the patient records that had also had the above mentioned surgery and had been referred by their orthopaedic surgeons for pain control and improved mobility.
On evaluation of this group of patients there was consistency with other studies in the comparison of their ages, gender and type of surgery with lateral epicondylitis surgery performed more frequently that medial epicondylitis surgery [1,5]. Unfortunately there was limited information in VAS and wound status in some of the patients but there was evidence of some patients requiring treatment many weeks after surgery, 16 weeks in one patient with the minimum referral being 10 days after surgery. There were a minimum number of treatments provided in one patient of two treatments and a maximum number of 12 treatments in another patient, with varying numbers of treatments in the others. Some of the wounds were oedematous and inflamed, most of the patients had limitation of extension of the elbow and there was only 50% resolution of the condition in these elbows according to the notes scrutinized. The treatments that were offered to these patients were usually multiple modalities that included ultrasound, electro-acupuncture, infrared laser, functional electrical stimulation, stretching, mobilization of the joint and exercises depending on the condition. These treatments would extend for longer than 20 min duration.
Although the incidence of neuropathic pain and or PPSP in elbow surgery is minimal yet chronic pain may be more common than realized. The condition could elicit chronic pain that may be due to pathogenic mechanisms that can be ascribed to preoperative, intra-operative and post-operative factors and that may produce ongoing complications for the patient and even neuropathic symp-toms. It was then decided to use this example of post-operative elbow surgery for treatment with a neurostimulator (Stimpod) that is minimal, non-invasive, of short duration and cost-effective and may prevent PPSP and relieve neuropathic symptoms.
In the results achieved the patients in the pilot study had some relief of severe and uncomfortable pain before the splint was removed and they required less medication than prescribed as it was given on an as needed basis. After the splint was removed pain levels increased as mobility improved but the pain increase was due to stretching of injured tissues with active movements and did not produce chronic and or spontaneous pain.
The most surprising effect was the movement that was already available immediately after the splint was removed and that continued to improve to full range without the usual treatment requiring mobilization, stretching and strengthening during rehabilitation.
The wounds also demonstrated minimal oedema and inflamma-tion that is not usually expected with recent surgery and continued to improve in some cases to an imperceptible scar. Scarring and sen-sitivity in the wound may augur chronic pain conditions and it is imperative to block pain and improve wound healing to prevent persistent pain and dysfunction.
By the last treatment patients had significantly improved and at one month after the last treatment the patients had almost all attained their goals of pain relief, range of movement and strength in their functional activities.
Patients were generally content with their progress in pain, movement and the type of treatment that was offered as it was of short duration, with a limited number of treatments required to achieve these results with minimal discomfort.
The neurostimulation device stimulated the brachial plexus in the first three treatments that then activates the specific nerve sup-ply affected by the operation, e.g. radial nerve superior and inferior to the elbow if a lateral epicodylitis surgery was performed. Initially this stimulation produced minimal fasciculation in the nerve but as the nerve conduction improved then activity within the nerve sup-ply became more evident with strong fasciculations occurring. This current could also translate in the opposite direction to the dorsal root ganglion of the cervical nerve roots.
When the splint was removed and the wound was exposed the neurostimulation was then applied to the radial nerve (in lateral epicondylitis surgery) superior and inferior to the elbow and to either end of the wound. The effect of this was increased fasciculations in the radial nerve and this even occurred with stimulation on the wound. Again the current would translate in the opposite direction to the brachial plexus and the dorsal root ganglion of the nerve involved.
The neurostimulation device that has been used in this case series appears to have effects on nerve conduction e.g. found in Bell’s palsy patients and relieves neuropathic pain from different aetiologies in many clinical situations since 2009 [12,20].
This type of neurostimulation was originally developed from a nerve-mapping device used by anaesthetists (2003) to detect a nerve before injecting and creating a nerve block prior to surgery. It was thought that to apply a magnetic field of 133 kHz to the square wave component of the nerve mapping current, a treatment would be developed that may be similar to that used in conventional pulsed radiofrequency (PRF) and that also included nerve mapping detection. In effect the current can target the nerve supply to an injury or damaged region. It is possible that nerve stimulation of the affected nerve may become a seminal treatment for blocking pain, normalizing nerve conduction with improvement in strength and range of movements. This treatment would there-fore be non-invasive and of short duration to create these healing effects.
In conventional PRF there is no destruction of the tissue involved (this could be at the dorsal root ganglion, among others) and it is the presence of the high frequency (pulsed 500 kHz) that improves nerve pain and dysfunction, albeit during an invasive procedure. It is also known that pulsed and continuous radio frequency adjacent to the dorsal root ganglion in a rat model induces latent cellular activity [22]. Neuroscientists measure expression of c-fos as an indirect marker of neuronal activity as c-fos is often expressed when neurons fire action potentials. Up-regulation of c-fos mRNA in a neuron indicates recent activity [23].
The neurostimulation provided to these patients demonstrated a capacity to decrease acute post-surgical pain, improve mobility and wound healing with treatment of short duration and minimal intervention by the physiotherapist. There was no sign of neuropathic symptoms in these patients 6 months post-surgery and any pain that was experienced could be attributed to a normal post-operative healing process and improvement in strength with functional activities. All patients were able to resume their normal function and sporting activities.
References:
- Shiri R, Vilkari-Juntura E, Varonen H, Heliovaara M. Prevalance and determinants of lateral and medial epicondylitis: a population study. Am J Epidemiol 2006;164(11):1065–74.
- Leach RE, Miller JK. Lateral and medical condylitis of the elbow. Clin Sports Med 1987;6(2):259–72.
- Tonks JH, Pai SK, Murali SR. Steroid injection therapy is the best conservative treatment for lateral epicondylitis: a prospective randomized controlled trial. Int J Clin Pract 2007;61(2):240–6.
- Stahl S, Kaufman T. The efficacy of an injection of steroids for medial epicondylitis. A prospective study of 60 elbows. J Bone joint Surg AM 1997;79(11):1648–52.
- Levin D, Levon NN, Miller TT, O’Kane PL, Feld RI, Parker L, et al. Lateral epicondylitis of the elbow: US findings. Radiology 2005;237(1), http://dx.doi.org/10.1148/radiol.2371040784.
- Bennet JB. Lateral and medial epicondylitis. Hand Clinic 1994;10:157–63.
- Jobe FW, Ciccotti MG. Lateral and medial epicondylitis of the elbow. J Am Acad Orthop Surg 1994;2(1):1–8.
- Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet 2006;367:1618–25.
- Poobalan AS, Bruce J, Smith W, Cairns S, King PM, Krukowski ZH, et al. A review of chronic pain after inguinal herniorrhaphy. Clin J Pain 2003;19(1):48–54.
- Kairaluroma PM, Bachmann MS, Rosenberg PH, Pere PJ. Preincisional paraverte-bral block reduces the prevalence of chronic pain after breast surgery. Anaesth Analg 2006;103:703–8.
- Haroutiunian S, Nikolajsen L, Finnerup NB, Jensen TS. The neuropathic com-ponent in persistent postsurgical pain: a systematic literature review. Pain 2013;154:95–102.
- Berger P. Electrical current and acupuncture treatment for a paediatric patient with a recurring long thoracic nerve paralysis. Acupunct Relat Ther 2014;2:14–8.
- Woolf CJ, Chong M-S. Preemptive analgesia-treating postoperative pain by preventing the establishment of central sensitization. Anaesth Analg 1993;77(2):362–79.
- Johansen A, Romundstad L, Nielsen CS, Schirmer H, Stubhaug A. Persistent postsurgical pain in the general population: prevalence and predictors in the Trompso study. Pain 2012;153:1390–6.
- Dualec C, Guastella V, Morand D, Cardot JM, Aublet-Cuvelier B, Mulliez A, et al. Characteristics of the neuropathy induced by thoracotomy: a 4-month follow-up study with psychophysical examination. Clin J Pain 2011;27:471–80.
- Bjordal JM, Johnson MJ, Ljunggreen L. Transcutaneous electrical nerve stimula-tion can reduce post-operative analgesic consumption in a meta-analysis with assessment of optimal treatment parameters for postoperative pain. Eur J Pain 2012;7:181–8.
- Johnson M. Transcutaneous electrical nerve stimulation; 2012, http://dx.doi.org/10.1002/9780470015902.a0024044 [Published online].
- Freynet A, Falcoz P-E. Control of post-thoracotomy pain by transcutaneous electrical nerve stimulation: effect on serum cytokine levels, visual ana-logue scale, pulmonary function and medication. Eur J Cardiothorac Surg 2012;41(4):861–8.
- Benedetti F, Amanzio M, Casadio C, Cavallo A, Cianci R, Giobbe R, et al. Con-trol of postoperative pain by transcutaneous electrical nerve stimulation after thoracic operations. Ann Thorac Surg 1997;63(3):773–6.
- Berger P. Intro NMS 460: a non-invasive pulsed radio frequency current for pain relief and nerve degeneration. Pretoria, South Africa: Xavant Technology; 2012.
- Vodovnik L, Karba R. Treatment of chronic wounds by means of electric and electromagnetic fields. Part 1. Literature review. Med Biol Eng Comput 1992;30:257–68.
- Van Zundert J, de Louw AJA, Joosten EAJ, Kessels AGH, Honig W, Dederen PJ, et al. Pulsed and continuous radio frequency adjacent to the dorsal root ganglion of rat induces latent cellular activity. Anesthesiology 2005;102(1):125–31.
- Dragunow M, Faull R. The use of c-fos as a metabolic marker in neuronal path-way tracing. J Neurosci Methods 1989;29(3):261–5.
Pain Management Centre, Guy’s & St. Thomas’ Hospitals
(United Kingdom)
External stimulation: simplistic solution to intractable pain
T. Goroszeniuk, S. Kothari
Pain Management Centre, Guy’s & St. Thomas’ Hospitals, London. SE1 7EH. UK
Introduction
Despite adopting a multidisciplinary approach, the management of neuropathic pain not infrequently presents a challenging clinical conundrum. Primary afferent stimulation for the control of chronic pain has been used widely during the last 40 years.
Current locations of access for stimulation include skin in Transcutaneous Electrical Nerve Stimulation (TENS) and acupuncture, peripheral nerve trunks, and primary afferent collaterals in the dorsal columns during Spinal Cord Stimulation (SCS). We have successfully investigated short external low-frequency stimulation either targetted at the site of the maximum pain or deeper afferent sensory nerves in patients with intractable painWe present the preliminary results of our study aimed at symptomatic relief and restoring function in patients with chronic, intractable pain.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Results
We noticed a dramatic reduction of the pain VAS. In 19 cases the VAS reduced to 0 at the end of 5 minutes demonstrating a 100% improvement in their pain status. The VAS scores decreased by 90% in four, 63% in another four and 50% in four more patients. The remaining three cases had their VAS score reduce by 25%, 20% and 15% respectively. In four patients with CRPS, vascular changes were observed at end of the procedure.
Conclusion
External stimulation is a noninvasive, simple and effective initial indicator, in patients with neuropathic pain, prior to longer, medium-term percutaneous stimulating catheter trial and subsequent implantation of permanent devices. The external application component allows the procedure to be performed on an outpatient basis and may be considered for diagnostic and repetitive therapeutic procedures. Further investigation is needed to establish a place for this technique in the management of chronic pain.
References:
- Alo K M., Holsheimer J., New trends in neuromodulation for the management of neuropathic pain. Neurosurgery, 2002, 4,690-704.
- Goroszeniuk T., Goroszeniuk D., Short neuromodulation trial in neuropathic pain produces varying duration but reproducible pain relief. Pain in Europe IV. 4th Congress of EFIC, Prague, 2-6.09.2003.
Case Reports
![]()
Case Reports
The reports listed in this section has shown such dramatic impact that practitioners using the Stimpod NMS460 felt compelled to share the results with us.
Electrical current and acupuncture treatment for a paediatric patient with recurring long thoracic nerve paralysis
By Prof. Phyllis Berger
Abstract
A female paediatric patient aged 9 years presented with right long thoracic nerve palsy for the second time. The first injury that occurred in 2011 was due to a fall and although the patient had a paralysis of the serratus anterior muscle and was unable to elevate the arm, with rehabilitation and conventional physiotherapy, she recovered completely according to the nerve conduction test that was conducted six months post-recovery.
The second injury to the long thoracic nerve was due to a ballet movement that occurred in 2012. Besides the nerve palsy that reoccurred, there was also a complication of severe pain and evidence of a complex regional pain syndrome (CRPS). The second injury was limited by the inability to participate in rehabilitation exercises and physiotherapy due to pain and hyperaesthesia in the distribution of C5 and C6 dermatome both in the trapezius and shoulder region. The third nerve conduction test deteriorated to those recorded after the first nerve conduction test.
A different physiotherapy approach was then applied – initially to reduce pain and decrease hyperaesthesia and then to attempt to increase nerve conduction by the inclusion of an electrical device that simultaneously delivers both a low and a high-frequency current. This treatment was combined with various pain resolving tactics including acupuncture, individual sub-liminal, low and high-frequency electrical currents. Several interventions were applied to tailor the treatment to the patient to achieve maximal improvement in pain and mobility. It is therefore difficult to attribute improvement to one particular modality or even natural resolution of the condition however previous clinical application and experience of activating nerve conduction with the combination current in other conditions implied that improvement could be expected. This particular electrical current is a combination of a low frequency and a magnetic field.
The condition resolved completely with full movement and no pain after 13 treatments over two months – it was evident that the combination of treatment had an effect on expediting the healing in the nerve. The patient was able to resume all her normal activities including gymnastics and ballet.
Report on a case series investigating a neurostimulation device for the treatment of pain and improvement of mobility and function following elbow surgery
Prof. Phyllis Berger & Jaye Jacks
Abstract
A group of seven patients received neurostimulation (Stimpod) post-tennis or golfer’s elbow surgery as their sole treatment to relieve acute post-operative pain, improve mobility and function. Patients undergoing the above-mentioned surgery have had chronic pain with and without neuropathic symptoms for a prolonged period. There is usually severe injury with active inflammatory processes due to the surgery. It was thought that treating these patients aggressively early post-operatively may expedite pain relief and the healing process.
Method
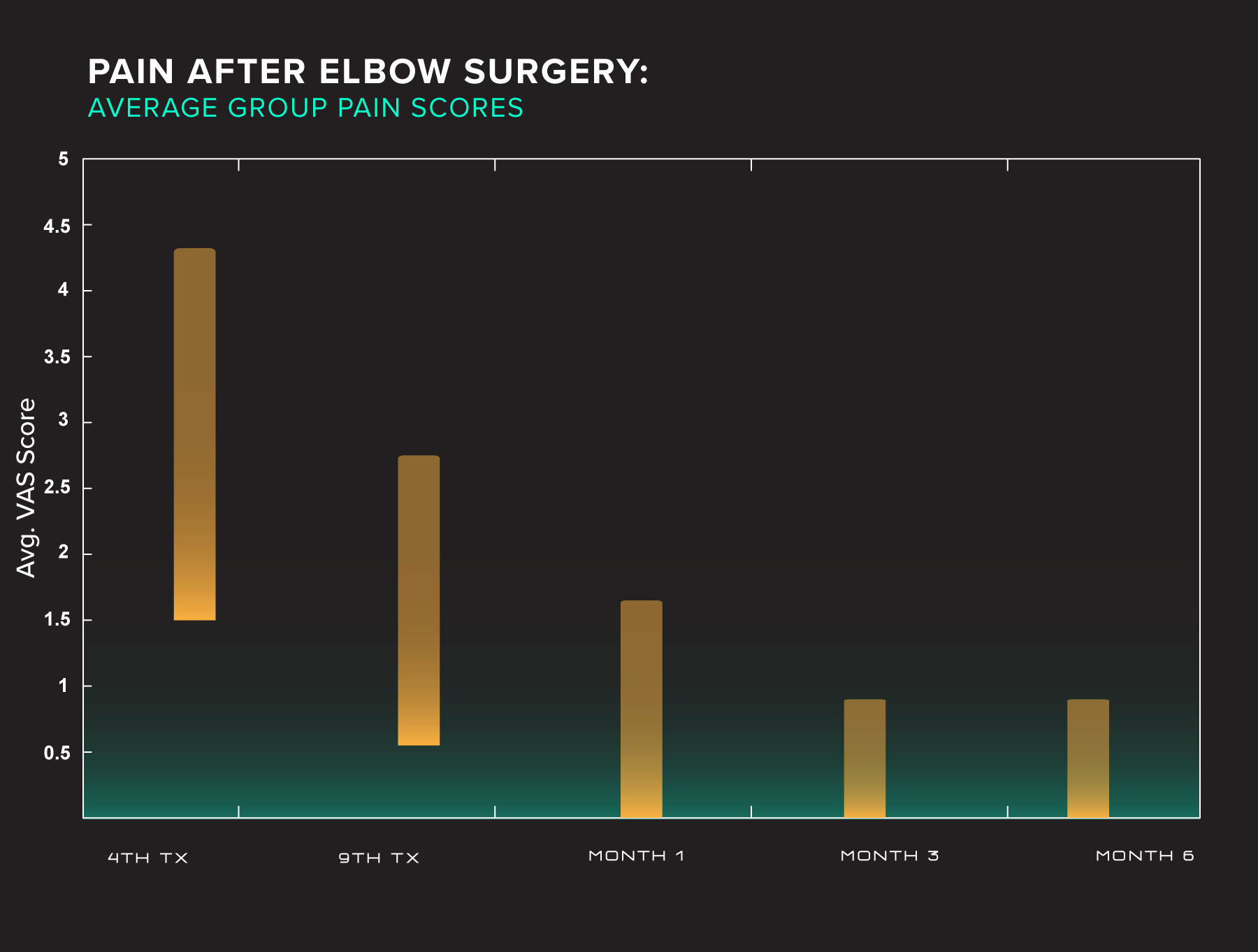
After their surgery, seven patients were given neurostimulation for three treatments of 20 min each on the brachial plexus during the 10 days before the splint was removed. This was followed by 6 treatments, twice weekly of 20 min each after the splint was removed. At each of these treatments 5-min stimulation were administered to four areas: the nerve supply (1) superior and (2) inferior to the elbow and (3 and 4) on either end of the wound. Patients were evaluated for pain with the visual analogue scale, movements of flexion and extension measured with a goniometer, strength and flexibility with a 12-movement activity scale, status of the wound and satisfaction with treatment, mobility and function. These measures were re-evaluated telephonically at one, three and six months after the last treatment.
Results
Significant pain relief was achieved by all of the seven patients before the splint was removed at the 4th treatment. Pain relief, range of movement and function was greatly improved at the final (9th) treatment by six of the seven patients and this was maintained with nearly full improvement of the above parameters for most of the participants at one month after the last treatment. Two patients had to have re-operation due to requiring more extensive surgery in the one patient and falling and injuring the original surgical site in the other patient. At three and six months after the last treatment full improvement in all the parameters above was maintained in the remaining five patients who also had excellent wound healing and satisfaction with their treatment, mobility and function.
Conclusion
It appears that the neurostimulation (Stimpod) has the capacity to improve acute post-surgical pain and reduce pain, improve mobility, function and stimulate wound healing once the splint was removed. This treatment is relatively cost effective, is non-invasive and of short duration. Positive effects were all maintained at 6 months.
The reports listed in this section has shown such dramatic impact that practitioners using the Stimpod NMS460 felt compelled to share the results with us.
Electrical current and acupuncture treatment for a paediatric patient with recurring long thoracic nerve paralysis
By Prof. Phyllis Berger
Abstract
A female paediatric patient aged 9 years presented with right long thoracic nerve palsy for the second time. The first injury that occurred in 2011 was due to a fall and although the patient had a paralysis of the serratus anterior muscle and was unable to elevate the arm, with rehabilitation and conventional physiotherapy, she recovered completely according to the nerve conduction test that was conducted six months post-recovery.
The second injury to the long thoracic nerve was due to a ballet movement that occurred in 2012. Besides the nerve palsy that reoccurred, there was also a complication of severe pain and evidence of a complex regional pain syndrome (CRPS). The second injury was limited by the inability to participate in rehabilitation exercises and physiotherapy due to pain and hyperaesthesia in the distribution of C5 and C6 dermatome both in the trapezius and shoulder region. The third nerve conduction test deteriorated to those recorded after the first nerve conduction test.
A different physiotherapy approach was then applied – initially to reduce pain and decrease hyperaesthesia and then to attempt to increase nerve conduction by the inclusion of an electrical device that simultaneously delivers both a low and a high-frequency current. This treatment was combined with various pain resolving tactics including acupuncture, individual sub-liminal, low and high-frequency electrical currents. Several interventions were applied to tailor the treatment to the patient to achieve maximal improvement in pain and mobility. It is therefore difficult to attribute improvement to one particular modality or even natural resolution of the condition however previous clinical application and experience of activating nerve conduction with the combination current in other conditions implied that improvement could be expected. This particular electrical current is a combination of a low frequency and a magnetic field.
The condition resolved completely with full movement and no pain after 13 treatments over two months – it was evident that the combination of treatment had an effect on expediting the healing in the nerve. The patient was able to resume all her normal activities including gymnastics and ballet.
Report on a case series investigating a neurostimulation device for the treatment of pain and improvement of mobility and function following elbow surgery
Prof. Phyllis Berger & Jaye Jacks
Abstract
A group of seven patients received neurostimulation (Stimpod) post-tennis or golfer’s elbow surgery as their sole treatment to relieve acute post-operative pain, improve mobility and function. Patients undergoing the above-mentioned surgery have had chronic pain with and without neuropathic symptoms for a prolonged period. There is usually severe injury with active inflammatory processes due to the surgery. It was thought that treating these patients aggressively early post-operatively may expedite pain relief and the healing process.
Method
After their surgery, seven patients were given neurostimulation for three treatments of 20 min each on the brachial plexus during the 10 days before the splint was removed. This was followed by 6 treatments, twice weekly of 20 min each after the splint was removed. At each of these treatments 5-min stimulation were administered to four areas: the nerve supply (1) superior and (2) inferior to the elbow and (3 and 4) on either end of the wound. Patients were evaluated for pain with the visual analogue scale, movements of flexion and extension measured with a goniometer, strength and flexibility with a 12-movement activity scale, status of the wound and satisfaction with treatment, mobility and function. These measures were re-evaluated telephonically at one, three and six months after the last treatment.
Results
Significant pain relief was achieved by all of the seven patients before the splint was removed at the 4th treatment. Pain relief, range of movement and function was greatly improved at the final (9th) treatment by six of the seven patients and this was maintained with nearly full improvement of the above parameters for most of the participants at one month after the last treatment. Two patients had to have re-operation due to requiring more extensive surgery in the one patient and falling and injuring the original surgical site in the other patient. At three and six months after the last treatment full improvement in all the parameters above was maintained in the remaining five patients who also had excellent wound healing and satisfaction with their treatment, mobility and function.
Conclusion
It appears that the neurostimulation (Stimpod) has the capacity to improve acute post-surgical pain and reduce pain, improve mobility, function and stimulate wound healing once the splint was removed. This treatment is relatively cost effective, is non-invasive and of short duration. Positive effects were all maintained at 6 months.
Literature Review
Literature Review
![]()
A selection of peer-reviewed scientific studies and clinical trials related to our technology and research.
A selection of research papers on Neuroplasticity, Peripheral (motor and sensory) and Cortical Recovery with a focus on patients with TBI and other head injuries
- Neuroplasticity in TBI Download PDF
- Peripheral recovery (motor and sensory) in TBI Download PDF
- Cortical recovery in TBI Download PDF
A selection of research on the treatment of Epilepsy, Depression, PTSD, Fibromyalgia, Multiple Sclerosis, Inflammation, Arthritis, Chronic Pain and Stroke with VNS.
- VNS for Epilepsy Download PDF
- VNS for Depression Download PDF
- VNS for Post Traumatic Stress Disorder Download PDF
- VNS for Fibromyalgia Download PDF
- VNS for Multiple Sclerosis Download PDF
- VNS for Inflammation Download PDF
- VNS for Rheumatoid Arthritis Download PDF
- VNS for Chronic Pain Download PDF
- VNS for Stroke Download PDF
- VNS for Adjunctive Treatments Download PDF
Introduction to PRF Research
Algiamed’s electromagnetic therapies utilize oscillating pulses in the radiofrequency spectrum, finding application in the treatment of osteogenesis, neurologically-related diseases and immune disorders.
Using non-invasive, cutting-edge technologies, Algiamed can deliver electromagnetic therapies which are targeted and well-tolerated.
The fast action and long-lasting effects of Algiamed’s electromagnetic therapies capitalize on the solid-state physics structures associated with bio-electronics. This cable-like conduction model delivers targeted electromagnetic fields along the nerves at a speed which is significantly faster than the conventional ionic flow model (i.e., action potentials).
The innovative action of Algiamed’s electromagnetic therapies on biological processes is best defined by the quantum interactions inside the body between our patented waveform and charged biological particles such as ions, atoms, and molecules.
Chronic and acute disorders are characterized by a change in the natural functionality of biological processes and are most often caused by a defect in mitochondrial genetic signaling leading to faults during cellular replication.
In the treatment of neuropathy, Algiamed’s goal is to identify the faults in the biological cascade that lead to pathological states. The treatment consists of applying an electromagnetic field aimed at correcting the biological cascade thus targeting the root cause of a patient’s neurologically-related disease. The ideal result leads to a long-lasting restoration of the intra-neural communication pathways and the natural nerve functionality.
A selection of peer-reviewed scientific studies and clinical trials related to our technology and research.
A selection of research papers on Neuroplasticity, Peripheral (motor and sensory) and Cortical Recovery with a focus on patients with TBI and other head injuries
- Neuroplasticity in TBI Download PDF
- Peripheral recovery (motor and sensory) in TBI Download PDF
- Cortical recovery in TBI Download PDF
A selection of research on the treatment of Epilepsy, Depression, PTSD, Fibromyalgia, Multiple Sclerosis, Inflammation, Arthritis, Chronic Pain and Stroke with VNS.
- VNS for Epilepsy Download PDF
- VNS for Depression Download PDF
- VNS for Post Traumatic Stress Disorder Download PDF
- VNS for Fibromyalgia Download PDF
- VNS for Multiple Sclerosis Download PDF
- VNS for Inflammation Download PDF
- VNS for Rheumatoid Arthritis Download PDF
- VNS for Chronic Pain Download PDF
- VNS for Stroke Download PDF
- VNS for Adjunctive Treatments Download PDF
Introduction to PRF Research
Algiamed’s electromagnetic therapies utilize oscillating pulses in the radiofrequency spectrum, finding application in the treatment of osteogenesis, neurologically-related diseases and immune disorders.
Using non-invasive, cutting-edge technologies, Algiamed can deliver electromagnetic therapies which are targeted and well-tolerated.
The fast action and long-lasting effects of Algiamed’s electromagnetic therapies capitalize on the solid-state physics structures associated with bio-electronics. This cable-like conduction model delivers targeted electromagnetic fields along the nerves at a speed which is significantly faster than the conventional ionic flow model (i.e., action potentials).
The innovative action of Algiamed’s electromagnetic therapies on biological processes is best defined by the quantum interactions inside the body between our patented waveform and charged biological particles such as ions, atoms, and molecules.
Chronic and acute disorders are characterized by a change in the natural functionality of biological processes and are most often caused by a defect in mitochondrial genetic signaling leading to faults during cellular replication.
In the treatment of neuropathy, Algiamed’s goal is to identify the faults in the biological cascade that lead to pathological states. The treatment consists of applying an electromagnetic field aimed at correcting the biological cascade thus targeting the root cause of a patient’s neurologically-related disease. The ideal result leads to a long-lasting restoration of the intra-neural communication pathways and the natural nerve functionality.
![]()